- Joined
- Jun 8, 2008
- Messages
- 54,197
"
By
Sandra Adamson Fryhofer, MD

This transcript has been edited for clarity.
Sandra Fryhofer, MD, highlights updates in the 2024 Advisory Committee on Immunization Practices (ACIP) Adult Immunization Schedule.
The biggest change for 2024 is that you don’t need to wait till January 1, 2024, for these schedules go into effect. Both schedules were published and became available in November 2023 and became effective immediately. They include ACIP recommendations approved by the Centers for Disease Control and Prevention (CDC) director through October 23, 2023.
Subsequent recommendations (before publication of the 2025 schedule) will be added to the addendum, a new Step 5, Section 5 in the schedule. The addendum should make Affordable Care Act (ACA)–compliant insurance plans cover ACIP-recommended immunizations sooner.
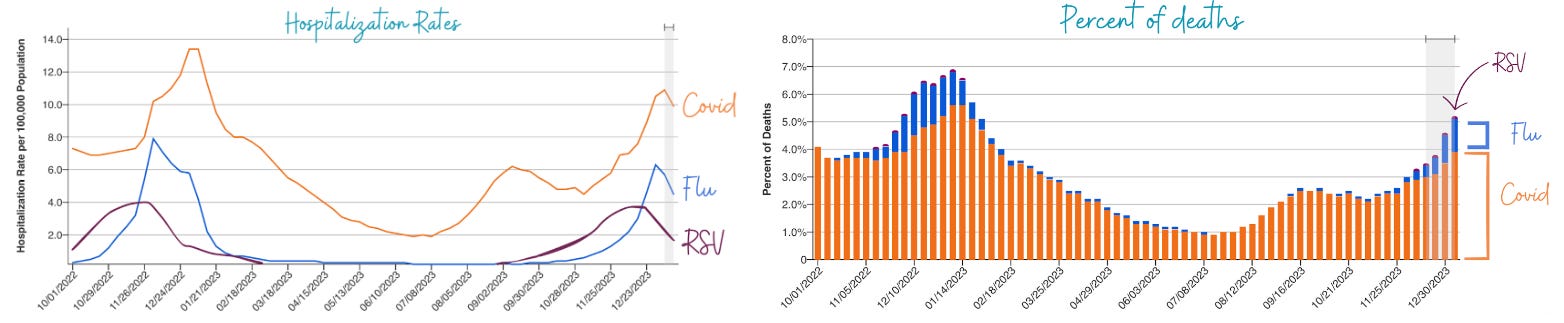
This year’s schedule includes more vaccines with new recommendations and new color code keys for the schedule’s vaccine tables. The newest vaccine additions to the 2024 schedule include respiratory syncytial virus (RSV) vaccines, the mpox vaccine (Jynneos), a new MenACWY-MenB combo vaccine (Penbraya), and the new 2023-2024 formulation of the updated COVID vaccine (both mRNA and protein-based adjuvanted versions).
These are listed on the cover page (in alphabetical order) by name, abbreviation, and trade name. Vaccine-specific details can be found in the (Step 3) Notes section, also organized alphabetically.
The order of and conditions covered in the columns on Table 2 have been reorganized.
Even for vaccines whose recommendations have not changed, the color code keys reflecting the recommendations have changed. For this reason, the 2024 version of Table 2 looks very different from the 2023 version. Also, much of the wording on overlays has been removed, which means you have to rely more heavily on the Notes section.
The color brown has been introduced on Table 2 to spotlight groups and conditions that require recurrent revaccination:
The rows for 2023-2024 formulations of COVID and flu vaccines are at the top of both tables are coded yellow, meaning everyone needs a dose of both vaccines.
Both tables have added a row for RSV vaccines and mpox vaccines.
COVID vaccines. The COVID vaccine note embraces the updated 2023-2024 formula. Everyone aged 6 months or older needs a dose of the updated COVID vaccine. Specifics of who needs what (and when) depend on what they have already received, as well as their immune status. Detailed recommendations for both mRNA and protein-based adjuvanted versions are included in the notes.
RSV vaccines. The notes also give vital details about RSV vaccines for pregnant people and for older adults. There are two RSV vaccines. Both are preF RSV vaccines. They’re identified by trade names for clarity. Arexvy contains an adjuvant. Abrysvo does not contain an adjuvant. The RSV vaccine note explains that only Abyrsvo (the vaccine without the adjuvant) can be given to pregnant people, only at 32-36 weeks, and only to those whose baby would be born during RSV season.
ACIP recommends a dose of either vaccine for adults aged 60 or older, under shared clinical decision-making (meaning you and your patients have to discuss and decide). The notes link to additional guidance for making that decision.
Mpox vaccines. For the mpox vaccine, all adults in any age group at increased risk of getting mpox should get a two-dose series of the vaccine. The mpox vaccine notes include a list of mpox risk factors.
With all these tools literally at your fingertips, there’s no reason not to know which vaccines your patients need and when. The challenge now is making it happen: getting those needed vaccines into arms.
"
"
The 2024 Adult Vaccine Schedule Changes Are Here
Publish date: December 27, 2023By
Sandra Adamson Fryhofer, MD
This transcript has been edited for clarity.
Sandra Fryhofer, MD, highlights updates in the 2024 Advisory Committee on Immunization Practices (ACIP) Adult Immunization Schedule.
The biggest change for 2024 is that you don’t need to wait till January 1, 2024, for these schedules go into effect. Both schedules were published and became available in November 2023 and became effective immediately. They include ACIP recommendations approved by the Centers for Disease Control and Prevention (CDC) director through October 23, 2023.
Subsequent recommendations (before publication of the 2025 schedule) will be added to the addendum, a new Step 5, Section 5 in the schedule. The addendum should make Affordable Care Act (ACA)–compliant insurance plans cover ACIP-recommended immunizations sooner.
This year’s schedule includes more vaccines with new recommendations and new color code keys for the schedule’s vaccine tables. The newest vaccine additions to the 2024 schedule include respiratory syncytial virus (RSV) vaccines, the mpox vaccine (Jynneos), a new MenACWY-MenB combo vaccine (Penbraya), and the new 2023-2024 formulation of the updated COVID vaccine (both mRNA and protein-based adjuvanted versions).
These are listed on the cover page (in alphabetical order) by name, abbreviation, and trade name. Vaccine-specific details can be found in the (Step 3) Notes section, also organized alphabetically.
The Tables
Step 1 is Table 1: Vaccinations by Age. Step 2 is Table 2: Vaccinations by Medical Conditions or Other Indications. The table names haven’t changed. However, their color code legends have been adjusted and refined. Also, the legends for the some of the same colors are not the same for both tables.The order of and conditions covered in the columns on Table 2 have been reorganized.
Even for vaccines whose recommendations have not changed, the color code keys reflecting the recommendations have changed. For this reason, the 2024 version of Table 2 looks very different from the 2023 version. Also, much of the wording on overlays has been removed, which means you have to rely more heavily on the Notes section.
The color brown has been introduced on Table 2 to spotlight groups and conditions that require recurrent revaccination:
- Give Tdap in each and every pregnancy at 27-36 weeks.
- Revaccinate people living with HIV with MenACWY every 5 years.
- Revaccinate those with asplenia and/or complement deficiency with MenACWY every 5 years and MenB every 2-3 years.
- Stem cell transplant recipients need three doses of Hib.
The rows for 2023-2024 formulations of COVID and flu vaccines are at the top of both tables are coded yellow, meaning everyone needs a dose of both vaccines.
Both tables have added a row for RSV vaccines and mpox vaccines.
Notes Section
The notes have been edited for clarity and reveal who needs what and when and include special vaccine-specific sections for special circumstances.COVID vaccines. The COVID vaccine note embraces the updated 2023-2024 formula. Everyone aged 6 months or older needs a dose of the updated COVID vaccine. Specifics of who needs what (and when) depend on what they have already received, as well as their immune status. Detailed recommendations for both mRNA and protein-based adjuvanted versions are included in the notes.
RSV vaccines. The notes also give vital details about RSV vaccines for pregnant people and for older adults. There are two RSV vaccines. Both are preF RSV vaccines. They’re identified by trade names for clarity. Arexvy contains an adjuvant. Abrysvo does not contain an adjuvant. The RSV vaccine note explains that only Abyrsvo (the vaccine without the adjuvant) can be given to pregnant people, only at 32-36 weeks, and only to those whose baby would be born during RSV season.
ACIP recommends a dose of either vaccine for adults aged 60 or older, under shared clinical decision-making (meaning you and your patients have to discuss and decide). The notes link to additional guidance for making that decision.
Mpox vaccines. For the mpox vaccine, all adults in any age group at increased risk of getting mpox should get a two-dose series of the vaccine. The mpox vaccine notes include a list of mpox risk factors.
Other Features of the 2024 Adult Immunization Schedule
The schedule has useful links to helpful information:- Vaccine information statements
- Complete ACIP recommendations
- CDC’s General Best Practice Guidelines for Immunizations.
- VAERS (CDC’s Vaccine Adverse Event Reporting System)
- Travel vaccination requirements
- Best practices guidelines for vaccinating persons with immunodeficiency
- The National Vaccine Injury Compensation program (for resolving any vaccine injury claims)
- CDC’s vaccine app
- QR code to access the schedule online.
With all these tools literally at your fingertips, there’s no reason not to know which vaccines your patients need and when. The challenge now is making it happen: getting those needed vaccines into arms.
"
"








![author['full_name']](https://assets.medpagetoday.net/media/images/author/2N5A0622_180.jpg "author['full_name']")


 | NIOSH | CDC")








![author['full_name']](https://clf1.medpagetoday.com/media/images/author/Faust_330px.png "author['full_name']")


300x240.png)